Issue Brief: Medications for Opioid and Alcohol Use Disorders: Research Insights for Criminal Justice Professionals
Key Takeaways
This Justice Community Opioid Innovation Network (JCOIN) issue brief provides a primer on FDA- approved medications to treat opioid use disorder (OUD) and alcohol use disorder (AUD).
OUD and AUD are complex conditions, and treatment must address biological, psychological, and social aspects of health. Medication may be one important piece of a comprehensive treatment and recovery support plan. Behavioral/psychosocial therapy in combination with medication can improve clinical outcomes. Medication should be coupled as needed and desired with behavioral treatment and supportive services such as stable housing, employment, peer navigators, and family or other social-support engagement [1].
An individual’s decision to decline counseling, or the absence of local behavioral treatment resources, should not preclude or delay the use of OUD or AUD treatment medication with appropriate medication management [2]. Buprenorphine and methadone have been shown to meaningfully reduce the risk of death, as well as decrease illicit opioid use, overdose, and serious opioid-related acute care [3]. Likewise, persons using opioids along with alcohol and other drugs (including cocaine and methamphetamine) can still benefit from medications for OUD and AUD, and these treatments can help reduce other polysubstance use.
Because methadone and buprenorphine are themselves opioids, some people have incorrectly asserted that the use of these medications is replacing one addiction with another. This misperception hinders the adoption of effective treatment options. Methadone and buprenorphine treat opioid withdrawal symptoms and pain. All three FDA-approved medications for OUD (methadone, buprenorphine, and naltrexone) reduce cravings and reduce or block the euphoric effects of illicit opioids. These treatments make it possible for people to engage in behavior-change activities and to function normally by participating in work, school, and other productive, prosocial life activities [4].
How These Medications Work
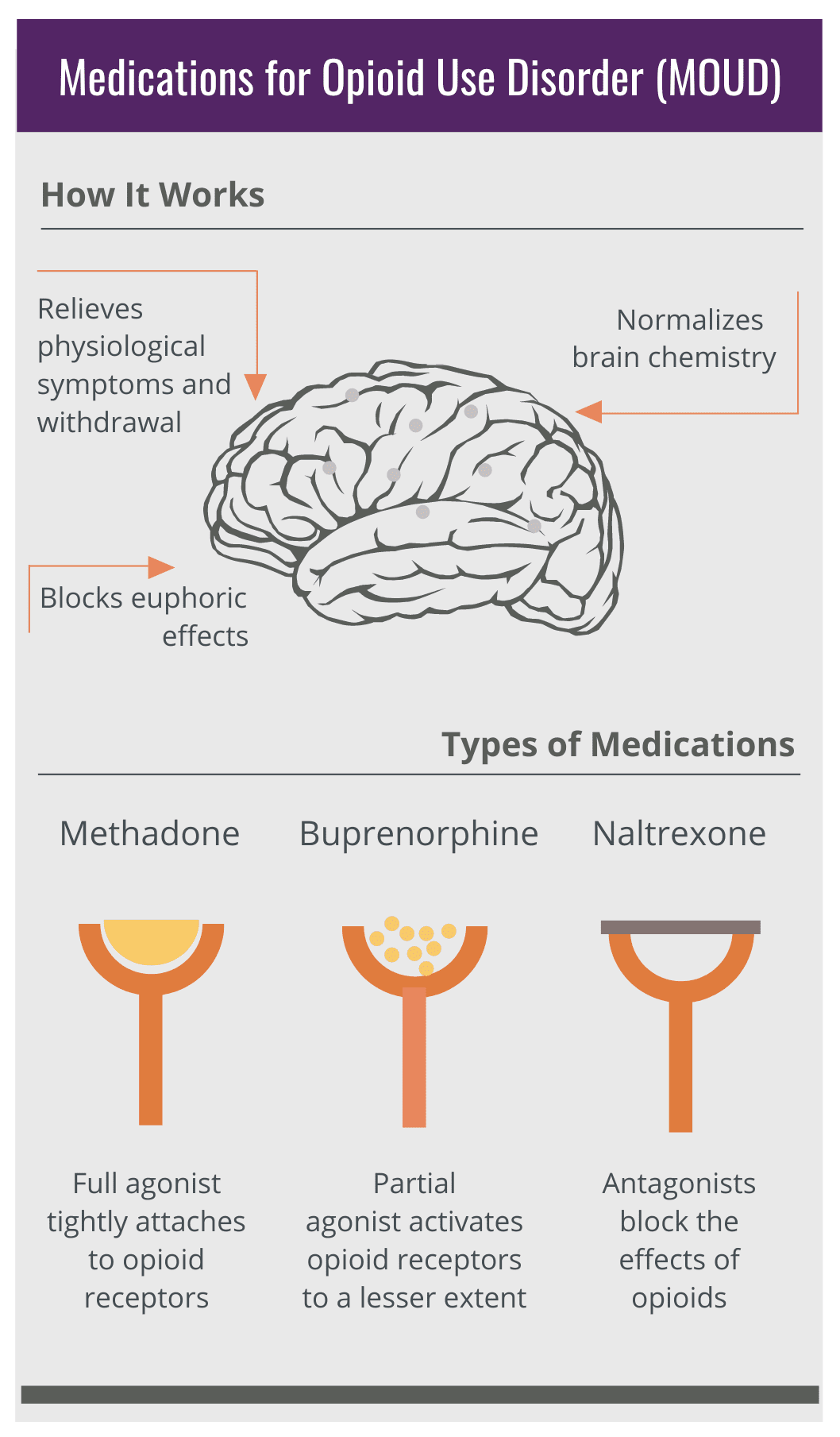
Source: Addiction Policy Forum Infographic [5]
Most of the medications for OUD and AUD work by binding to specific receptors in the brain. Receptors are part of the central nervous system. Different receptors react to different kinds of stimuli, such as temperature, pressure, light, or chemicals.
Methadone, buprenorphine, and naltrexone bind to opioid receptors. Depending on how they bind to receptors and the effect they cause, medications for opioid use disorder are classified as an agonist (methadone), partial agonist (buprenorphine), or antagonist (naltrexone). An agonist is a drug that binds to and activates certain receptors in the body. Opioid agonists work by acting on opioid receptors in the brain. A partial agonist is a drug that binds to and activates certain receptors, but to a lesser extent than full agonists. Partial opioid agonists work by acting on opioid receptors in the brain but activate them less strongly than full agonists. An antagonist is a drug that binds to certain receptors without activating them.
Opioid antagonists work by blocking the activation of opioid receptors.
Alcohol stimulates different receptors, called GABA receptors, in the brain. Though naltrexone binds to the opioid receptor, and not to the GABA receptor, it can help reduce cravings and alcohol intake in treatment of AUD, probably because of the critical role of the opioid receptor in the brain’s reward system.
Acamprosate binds to different receptors in the brain. Although the precise mechanisms of action of acamprosate are not yet known, it appears to help in the modulation of a neurotransmitter system that is affected by alcohol consumption.
Unlike the other medications discussed here, disulfiram does not directly affect receptors in the brain. Instead, it blocks enzymes that the body uses to break down alcohol.
It should be noted that none of the AUD medications treat the symptoms of acute alcohol withdrawal, which can be severe, life threatening, and may require hospitalization.
Medications for Opioid Use Disorder
Medications for opioid use disorder (particularly methadone and buprenorphine) have been proven to help reduce opioid use and opioid use disorder-related symptoms, the risk of infectious disease transmission, and criminal behavior associated with drug use. These medications increase the likelihood that a person will remain in treatment. They also mitigate the risks of overdose and death, particularly when used with a comprehensive treatment and recovery support plan [6,7,8,9].
Generic Name: Methadone
Related Brand Names: Diskets®, Dolophine®, Methadone Hydrochloride Intensol™, Methadose™
Pharmacology: Methadone is a synthetic opioid agonist that blunts or blocks the intoxicating effects of other opioids such as heroin. It reduces withdrawal symptoms and cravings. When properly administered to someone who is physiologically tolerant to opioids, there are no intoxicating effects. Methadone does cause physiological dependence, including the potential for overdose. Methadone is safe and effective when taken as prescribed.
Form: Methadone can be dispensed in liquid form or a pill.
Prescription and Administration: Methadone must be ordered by a qualified medical professional and directly administered or dispensed (as take-home doses) in a federally regulated and accredited opioid treatment program (OTP). Federal regulations require counseling for people receiving methadone. Some rules for administering methadone, such as the use of telehealth and take-home doses, were temporarily changed in response to COVID-19. Methadone take-home doses can be dispensed in a maximum of 28-day supplies for very stable patients. The Substance Abuse and Mental Health Services Administration provides guidance for OTPs, including regulation changes made in response to COVID-19 [10]. Jails and prisons can be certified as OTPs or work with community-based OTPs.
Generic Name: Buprenorphine
Related Brand Names: Suboxone®, Sublocade®, Zubsolv®, Bunavail™
Pharmacology: Buprenorphine is a partial opioid agonist that partially stimulates opioid receptors while blocking the effects of other opioids such as heroin. It treats withdrawal symptoms, cravings, and pain, and has less risk of respiratory suppression than full opioid agonists. Because it is an opioid, it does cause physiological dependence, and will have opioid effects in individuals who are opioid-naive or who have lost opioid tolerance. Buprenorphine is safe and effective when taken as prescribed.
NOTE: Suboxone, Zubsolv, and Bunavail contain a combination of buprenorphine and naloxone. Naloxone is an overdose-reversal medication commonly found under the brand name Narcan. The naloxone in this combination product is present to reduce the likelihood of misuse. This is the most prescribed formulation of buprenorphine.
Form: Buprenorphine can be dispensed as a sublingual tablet or buccal film. It is also available as a monthly injection, or a subdermal implant that lasts for six months.
Prescription and Administration: Buprenorphine must be prescribed and administered by a qualified medical professional who has completed a required training course and received a specific federal license to prescribe it.
Generic Name: Naltrexone
Related Brand Names: Vivitrol®, ReVia®, Depade®
Pharmacology: Naltrexone is an opioid antagonist that blocks the intoxicating effects of opioids without stimulating the opioid receptors. It does not reduce withdrawal symptoms and in fact will precipitate withdrawal in individuals who are opioid dependent and have not been abstinent from opioids for an adequate amount of time (typically 7 days for short-acting opioids and 10–14 days for long-acting opioids). It does not cause intoxication or physiological dependence. Naltrexone is approved for relapse prevention in patients with opioid use disorder.
Form: Naltrexone comes in an extended-release monthly injection, or as a daily tablet. In OUD, the long-acting monthly injectable formulation of naltrexone is FDA approved for relapse prevention, but the oral formulation of naltrexone is not effective for the treatment of OUD and should only be used prior to starting the injectable formulation [11,12].
Prescription and Administration: Naltrexone must be prescribed by a licensed medical practitioner. The injectable formulation can be administered by a licensed provider such as a nurse or pharmacist.
A Note on Naloxone
Naloxone is not used to treat opioid use disorder, but it is critical as an emergency medication to prevent death from overdose. It is an FDA-approved medication to quickly reverse opioid overdose. Naloxone is commonly found under the brand name Narcan.
Medications for Alcohol Use Disorder
Medications to treat alcohol use disorder (naltrexone, acamprosate, and disulfiram) have been proven to help reduce alcohol consumption [13,14]. None of the medications summarized here are treatments for acute alcohol withdrawal, which may be severe, life-threatening, and require emergency room or inpatient care.
Generic Name: Naltrexone
Related Brand Names: Vivitrol®, ReVia®, Depade®
Pharmacology: Naltrexone is an opioid antagonist that attenuates the euphoric effects of alcohol on the body and reduces alcohol cravings. The mechanisms by which naltrexone induces the reduction in alcohol consumption are not entirely understood. It does not reduce withdrawal symptoms.
Form: For AUD, naltrexone can be administered as an extended-release monthly injection or administered or dispensed as a tablet.
Prescription and Administration: Both forms of naltrexone can be prescribed by any licensed medical practitioner and administered by medical providers, nurses, or pharmacists.
Generic Name: Acamprosate
Related Brand Names: Campral®
Pharmacology: Acamprosate has agonist and antagonist effects on different receptors in the body. The precise mechanisms of action of acamprosate are not yet known. Acamprosate does not prevent withdrawal symptoms, but it can reduce the negative symptoms associated with the period immediately following alcohol withdrawal.
Form: Acamprosate is dispensed as a tablet.
Prescription and Administration: Acamprosate can be prescribed and administered by any licensed medical practitioner
Generic Name: Disulfiram
Related Brand Names: Antabuse®
Pharmacology: Unlike other medications approved to treat alcohol use disorder, disulfiram does not directly affect receptors in the brain. Instead, it blocks enzymes in the body that break down alcohol. If alcohol is ingested by someone taking disulfiram, it can cause nausea, flushing, and heart palpitations.
Form: Disulfiram is dispensed as a tablet.
Prescription and Administration: Disulfiram can be prescribed and administered by any licensed medical practitioner.
Glossary
Medications for Addiction Treatment (MAT): MAT refers to addiction treatment involving the use of FDA-approved medications. MAT is sometimes used as an abbreviation for “medication-assisted treatment”; however, this term reinforces the misconception that counseling alone is a treatment and medication only “assists” the counseling; this can worsen stigma around opioid use [15]. Medications are treatment. Many health conditions (hypertension, diabetes) are treated with medications, without using the word “assisted.”
Medications for Opioid Use Disorder (MOUD): MOUD refers to FDA-approved medications that are used to treat opioid use disorder.
Agonist: An agonist is a drug that binds to and activates certain receptors in the body. Opioid agonists work by acting on opioid receptors in the brain. Methadone is an opioid agonist.
Partial Agonist: A partial agonist is a drug that binds to and activates certain receptors, but to a lesser extent than full agonists. Partial opioid agonists work by acting on opioid receptors in the brain but activate them less strongly than full agonists. Buprenorphine is a partial opioid agonist.
Antagonist: An antagonist is a drug that binds to certain receptors without activating them. Opioid antagonists work by blocking the activation of opioid receptors. Naltrexone and naloxone are opioid antagonists.
For More Information
National Institute on Alcohol Abuse and Alcoholism (NIAAA): Treatment for alcohol problems: Finding and getting help
National Institute on Drug Abuse (NIDA): Effective treatments for opioid addiction
National Institute on Drug Abuse (NIDA): Treating opioid addiction in criminal justice settings
National Institute on Drug Abuse (NIDA): Treatment approaches for drug addiction
Substance Abuse and Mental Health Services Administration (SAMHSA): Use of medication-assisted treatment for opioid use disorder in criminal justice settings
Substance Abuse and Mental Health Services Administration (SAMHSA). Medication for the treatment of alcohol use disorder: A brief guide
References
[1] Hamilton, L., & Belenko, S. (2015). Effects of pre-release services on access to behavioral health treatment after release from prison. Justice Quarterly, 33(6), 1080–1102. https://doi.org/10.1080/07418825.2015.1073771
[2] American Society of Addiction Medicine. (2020). National practice guideline for the treatment of opioid use disorder: 2020 focused update. Journal of Addiction Medicine, 14(2S), 1–91. https://doi.org/10.1097/adm.0000000000000633
[3] Wakeman, S. E., Larochelle, M. R., Ameli, O., Chaisson, C. E., McPheeters, J. T., Crown, W. H., Azocar, F., & Sanghavi, D. M. (2020). Comparative effectiveness of different treatment pathways for opioid use disorder. JAMA Network Open, 3(2). https://doi.org/10.1001/jamanetworkopen.2019.20622
[4] National Institute on Drug Abuse. (2021, June). What are misconceptions about maintenance treatment? https://www.drugabuse.gov/publications/research-reports/medications-to-treat-opioid-addiction/what-are-misconceptions-about-maintenance-treatment
[5] Addiction Policy Forum. (2020). How the medications work to treat opioid use disorder [Infographic]. Navigating addiction and treatment: A guide for families. https://www.addictionpolicy.org/post/navigating-treatment-and-addiction-a-guide-for-families
[6] National Institute on Drug Abuse. (2018, June). How effective are medications to treat opioid use disorder? https://www.drugabuse.gov/publications/research-reports/medications-to-treat-opioid-addiction/efficacy-medications-opioid-use-disorder
[7] National Institute on Drug Abuse. (2018, June). How is opioid use disorder treated in the criminal justice system? https://www.drugabuse.gov/publications/research-reports/medications-to-treat-opioid-addiction/how-opioid-use-disorder-treated-in-criminal-justice-system
[8] Substance Abuse and Mental Health Service Administration. (2019). Use of medication-assisted treatment for opioid use disorder in criminal justice settings. U.S. Department of Health and Human Services. https://store.samhsa.gov/sites/default/files/d7/priv/pep19-matusecjs.pdf
[9] National Commission on Correctional Health Care. (2016, October 23). Substance use disorder treatment for adults and adolescents. https://www.ncchc.org/substance-use-disorder-treatment-for-adults-and-adolescents
[10] Substance Abuse and Mental Health Service Administration. (2021, August 27). Coronavirus (COVID-19): Guidance for OTPs. https://www.samhsa.gov/coronavirus
[11] Minozzi, S., Amato, L., Vecchi, S., Davoli, M., Kirchmayer, U., & Verster, A. (2011). Oral naltrexone maintenance treatment for opioid dependence. Cochrane database of systematic reviews, 2011(4), CD001333. https://doi.org/10.1002/14651858.CD001333.pub4
[12] National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Sciences Policy; Committee on Medication-Assisted Treatment for Opioid Use Disorder, Mancher, M., & Leshner, A. I. (Eds.). (2019). Medications for Opioid Use Disorder Save Lives. National Academies Press (US). https://www.ncbi.nlm.nih.gov/books/NBK541393/
[13] National Institute on Alcohol Abuse and Alcoholism. (2021, March). Treatment for alcohol problems: Finding and getting help. U.S. Department of Health and Human Services, National Institutes of Health. https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/treatment-alcohol-problems-finding-and-getting-help
[14] Substance Abuse and Mental Health Services Administration & National Institute on Alcohol Abuse and Alcoholism. (2015). Medication for the treatment of alcohol use disorder: A brief guide. U.S. Department of Health and Human Services. https://store.samhsa.gov/product/Medication-for-the-Treatment-of-Alcohol-Use-Disorder-A-Brief-Guide/SMA15-4907
[15] American Psychological Association. (2019, June). How to talk about addiction. Monitor on Psychology, 50(6). http://www.apa.org/monitor/2019/06/cover-opioids-talk-sidebar
This Issue Brief was developed by TASC in conjunction with JCOIN’s Medications for Opioid Use Disorder Workgroup. This activity was funded under a subcontract to the JCOIN Coordination and Translation Center (U2CDA050097). JCOIN is funded by the National Institute on Drug Abuse as part of the NIH HEAL Initiative. The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of the NIH, the NIH HEAL Initiative, or the participating sites.
Suggested citation: Rodriguez, P., Charlier, J., Baille, D., Baumgartner, L., Whitney, T., and the JCOIN MOUD Workgroup. (2021). Medications for Opioid and Alcohol Use Disorders: Research Insights for Criminal Justice Professionals [JCOIN Issue Brief #2]. https://www.jcoinctc.org/issue-brief-medications-for-opioid-and-alcohol-use-disorders/